Applying to Emergency Medicine Residency
So you’re interested in going into emergency medicine, the single best specialty? You’ve come to the right…


So you’re interested in going into emergency medicine, the single best specialty? You’ve come to the right place: in this blog post, I’ll share my highly *unbiased* thoughts on why EM is the greatest, and give some tips on things to know about applying to EM residency in the United States (especially as an international medical graduate aka IMG).
Why I Love Emergency Medicine:
If you’re wondering why one would even apply to EM residency, here is my list. The reasons are innumerable, but I’ll try to keep my excitement in check and focus on the main ones**:
- Incredibly varied day-to-day: no two days are the same, from your schedule to your team members to your patients.
- Great mix of hands-on skills and theoretical knowledge: EM is very procedural, from intubations to central line placements to draining abscess, but you never forget the “real” medicine because you’re kept on your toes by strange presentations of everyday diseases.
- Instant gratification: have a suspicion that your patient might have an aortic dissection or worried that they might have severe anemia? Order your tests and get same-day answers. Bedside ultrasound is a great tool and incredible skill to train: if you suspect your patient has a pericardial effusion, you grab the US probe and take a quick look: 3 minutes later and you’ve got your answer!
- Solve puzzles: the mystery of the undifferentiated patient – you work very fast, with very little information, usually on a time crunch.
- Shift work: there’s no feeling more glorious than being off on a random Tuesday, while the rest of the world is hard at work. I’ve got a lot to say on shiftwork so scroll down to see below!
There’s more!
- Leave work at work: when you go home, you never have to prep for next day’s cases or follow up on your patients (unless you want to — and we all definitely do!). You sign your patients out at the end of the shift and another team takes over and you’re free to go home and unwind.
- FOAMed: the world of emergency medicine is one of the fastest evolving fields and there is a constant strive for using evidence-based medicine. FOAMed stands for Free Open-Access Medical Education, and the internet is FULL of podcasts, blog posts, articles, aimed at teaching and sharing knowledge about the latest research. The concept of “we do this because it’s how we’ve always done it” is fading in EM and I’m all for it.
- Moonlighting: it’s very common in EM to be allowed to work at a different facility (or within your own facility) after the first year of residency as a moonlighter, and make more money while also learning more about how institutions are run. The rate I’ve heard is $70/hour when you’re moonlighting, but there are of course restrictions (work hours, good standing as a resident, etc.).
- Different types of EDs make for different experiences: you can work at a ‘free standing’ ED, or single provider ones; you can work at a large community hospital or at an academic center. You can work as a faculty member at a residency program and enrich the lives of the residents (aww), or choose to work per diem at two or three different places to keep your skills up.
- Work with the underserved: not everyone has access to healthcare unfortunately, and many of them end up in the ED looking for primary care. While it’s not ideal, it does happen a lot and managing these patients require a certain skill – how to best help your patients who have very poor followup.
- Save lives… that feeling when you are resuscitating a dead person and get ROSC — only to follow up two weeks later after their ICU stay to learn that the patient had good neurological outcome? Nothing comes close for me. You also save lives in less indirect ways, and the patients are often so grateful.
- Be there for someone’s “worst day of their life”: whether you have to give a presumptive cancer diagnosis, or tell a family that their grandmother has passed, or let a mom-to-be know that she lost her baby… the way you do it matters. Your patients are vulnerable and hurting and you are their doctor: it’s an unparalleled privilege.
**As I was writing this blog post, more and more things popped into my head, and my original “five things I love about EM” quickly became this monstrosity.
The Beauty of Shiftwork
Your days are varied; here’s an example of two weeks in emergency medicine (as a resident!*). These two weeks are a bit unusual because we had a resident retreat scheduled for one of the weekends — usually we do a row of 6 nights from Wednesdays to Monday.
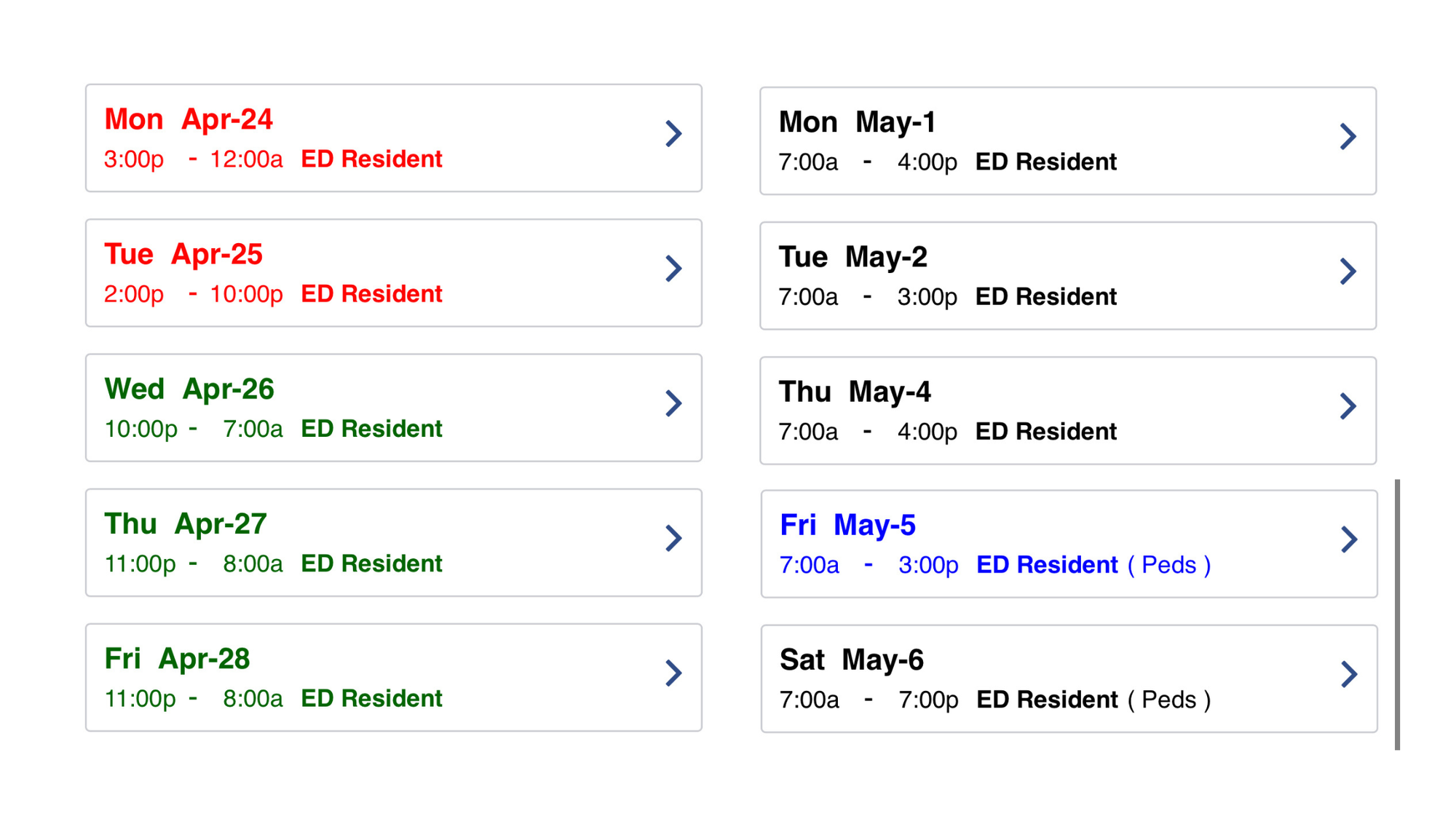
You can go to the dentist without taking a “personal” day off and take care of your errands. Some days you’ll work mornings, then some nights, maybe an afternoon here or there. Each ED has different lengths of shifts – some work 8 hour shifts, some 9 or 10 or 11 or 12. You can figure out which you like best and choose that as your attending job.
I personally like 9-10 hour shifts; I have time before or after to work out and don’t feel completely exhausted. 12s are nice in the sense that you have to work fewer days a month.
*Keep in mind that schedules as an attending are very different — and you’re much more free to choose preferences.)
As an attending, you can choose how many shifts you want to work, and switch shifts with a coworker if some life event comes up (i.e. your child has a field trip you want to chaperone). The attending I babysat for worked 8 days a month and that was it; another attending I work with works 20 shifts a month. One attending stacks his monthly shifts in the first two weeks and travels in the second two weeks. I’ve met a few moms who choose to work nights so that they can take their children to school in the morning, sleep while they’re at school, and be awake by the time they get up. You can work full-time or “per diem” — the combinations and options are endless. It’s up to you!
Applying to EM Residency
So now that you’re convinced that EM is the only specialty for you, what next?
Depending on what stage you’re in in your academic journey, the specifics might be different, but the answer all leads to this one central concept:
Put together an EM residency application that shows a passion for emergency medicine above all.
Prove that no other specialty will do for you.
As I like to say: your application should demonstrate (show, don’t tell) that all roads lead to emergency medicine.
What do I mean by that?
Everything, from your extra-curriculars to your research to your clinical experience, should cohesively point towards emergency medicine. For instance, if you say that you care about the underserved, show that you’ve actually worked with them in the past and it’s not just lip service.
If you say you’re passionate about global health – how does your application reflect that? Have you traveled or joined a club or done research?
CORE COMPONENTS OF YOUR EM RESIDENCY APPLICATION
Personal Statement
Some program directors (PDs) care a lot about the PS; others have straight out said that they don’t read them. My tip is to write one – have a friend read it – rewrite it/fix it – have someone else read it, and so on. There’s no point in obsessing over it though; it is just a short essay.
I read a lot about how to write a great PS, and I was complimented on mine during a few interviews. The general format that I was recommended to follow was:
- hook: catch their attention with a great opener.
- why EM: explain why you’re applying to this specialty.
- why you: what makes you a good candidate for this program? Think of this as an elevator pitch promoting yourself.
Some other important notes:
- Do not have any spelling mistakes, not a single one. It just looks bad.
- Do not go over 1 page (some people say it’s okay to have an extra line or two, but most agree that you should stick to the one-page limit).
- Do use the uploader once you get your token to make sure you fit within the limit of 1 page (it’s different than a page in Word).
- Do start early, but like I said: don’t obsess.
- Do have people read it over; preferably a mentor, but a parent could do too. If you have lots of friends, as a few different people for input, but don’t feel the need to take all their suggestions.
- If personalizing your PS, do NOT send it to the wrong program by accident.
Please don’t feel the need to send a personalized PS to each program; that would be incredibly time-consuming. Although it’s becoming a more common practice (one program specifically asked for a personalized PS, so I obliged), it still okay to send a generic one. One thing I did do was create two generic versions of the same PS, one for “far away” programs, and ones on the East Coast. Since I could imagine myself matching and being happy either close or far from home, I tailored the PS and sent it to the appropriate distinct groups. I also wrote personalized PS for my top 3-5 programs.
I used a website to read through some sample personal statements, but I actually can’t find that link, so I found this instead for you guys: MD Personal Statements.
SLOE
The SLOE (pronounced “slow,” apparently, and not “slow-y”, whoops) is unique to emergency medicine and a few specialties. SLOE stands for Standardized Letter of Evaluation, because instead of a regular letter of recommendation (LOR), it asks faculty to evaluate your performance as it compares to other students’. The SLOE was meant to make LORs more objective… and while I agree with the sentiment behind it, unfortunately I recognize that the SLOE is definitely not perfect.
That being said, it is one of the most highly regarded parts of the application. A SLOE can make or break your foray into the world of EM (which is a little scary), and it’s important to get a good one. You receive a SLOE after doing a rotation in emergency medicine; more on that later.
For starters, understanding the different types of SLOEs is useful. If you go to the official website, they have an explanation (CORD SLOE); otherwise, EMRA and some of the other EM mentoring websites do seminars on the different kinds.
The eSLOE is the most powerful one: it’s the one written by a faculty member at an EM residency. These are highly coveted — and very very difficult for IMGs to obtain. I personally would not have applied without an eSLOE (I was a nervous applicant), but I did have a friend who never set foot in the US and still matched into EM without any personal contacts. So it’s doable, but tough.
If you’re unable to obtain an official SLOE, you should have your letter writers use the SLOE format; it’s better than using the unstandardized, slightly rambling LOR that most specialties work with.
SLOEs are comparing you to your peers, so it’s important to do well. Please listen to this podcast prior to starting your EM rotation: it’s fantastic and helped me a lot.
How to Crush Your SLOE by EM CLERKSHIP Podcast
ROTATIONS
it’s great to have some EM experience under your belt; not just for the SLOE, but also because it rounds out your application and it can help convince you that this is indeed the specialty that you want to dedicate your life to.
US medical students usually did two away rotations (and one home EM rotation) prior to COVID. During the pandemic, the recommendation was for a total of two away rotations — that might change with each year. Planning for two rotations is definitely useful; it’s expensive (because of the travel and housing), but it’s worthwhile. You get to see what different residencies are like, you get facetime with the faculty at two+ programs, and you learn more about why you love EM.
Again, listen to the podcast series above on how to do well on your rotation and secure a great SLOE.
Also, here is my link to some tips on how to secure a US clinical rotation (it’s really hard as an IMG), which is essential for your EM residency application.
GET INVOLVED
Show your passion for EM by becoming part of the EM community. Here are some easy ways to do so:
- join the national organizations (I am a part of EMRA/ACEP and AAEM; membership is free for US students and cheap for international students/graduates). They offer webinars, mentorship, resources and so much more.
- attend a conference: if you have the time and money, try to go to one of the big national conferences; they’re a great learning opportunity and networking event. They usually offer mentorship and application advice too!
- join a committee or become a young leader in EM: these organizations are always announcing different ways to get involved in leadership – follow them on Twitter or sign up for their newsletter
- join the world of #MedTwitter: create a professional Twitter account and connect with the orgs (EMRA, AAEM, SAEM), residency programs, and #embound peers
- write for a blog! become a contributor as a medical student; one that I love is i-em.org (international emergency medicine), which is always looking for bloggers and has an incredible volunteer team working on the website and even a book
- start research projects and get published: this one is arguably the most difficult (check out my other blog posts on research and networking)
Many of these are things you can do remotely, and it’s important to start early.
So there you have it. Those are my tips for applying to EM residency. If you have additional suggestions, please comment them.
Good luck with your EM residency application, and if you’d like my thoughts on the EM job market – let me know!


